- The biggest predictor of the need for breast implant revision is a failed previous revision. Many patients come to me after a series of previous operations, often by experienced plastic surgeons, but the problem was made worse with each surgery. In order to avoid getting on this cycle of revisions, make sure you understand the surgeon’s explanation of the problem and the plan to fix it.
- Don’t be tempted to take shortcuts. An example of this is trying to avoid having a breast lift by using large implants. If the skin envelope has been expanded from prior breast feeding or other reasons, the volume required to fill it up may be more than it can support. No one wants the scars of a breast lift, but you may end up with even more sagging and need a bigger lift later.
- Understand the limits of your individual anatomy; the implants cannot be wider than the breast (base diameter), and implants too large for your frame will cause problems that can be difficult to correct.
- Consider adding support with an internal bra. Implants that have bottomed out, fall to the sides when you lie down, or show rippling, may lack coverage and support. An internal bra is not simply suturing the scar capsule with permanent sutures; it is the addition of a layer of support. Gala mesh and ADM such as Strattice work well for this.
 Correction of animation deformity and Strattice Internal bra (patient flexing)
Correction of animation deformity and Strattice Internal bra (patient flexing) - Don’t do the same thing again hoping for a different result. This comes up a lot when patients are seeing me for treatment of animation deformity, which is caused by releasing (cutting) the attachments of the pectoral muscle from the rib cage with under muscle placement using the dual plane method. Surgeons often just release the muscle more, making the problem worse. The solution is to re-attach the muscle, by converting to split muscle or dual plane.
- A second (or third) opinion can often bring fresh perspective on the issue, especially if there has been a failed revision already. The success stories I am the most proud of are the ones where I was the 10th plastic surgeon consulted, but the first to offer an explanation of the problem that made sense to the patient and a different plan.
- Once you have found a surgeon that you think is the right one, don’t second-guess their recommendations based on advice from friends or “Dr. Google”. Revision breast surgery is complicated and there is a lot of misinformation floating around.
- Experience counts more than marketing or social media prominence.
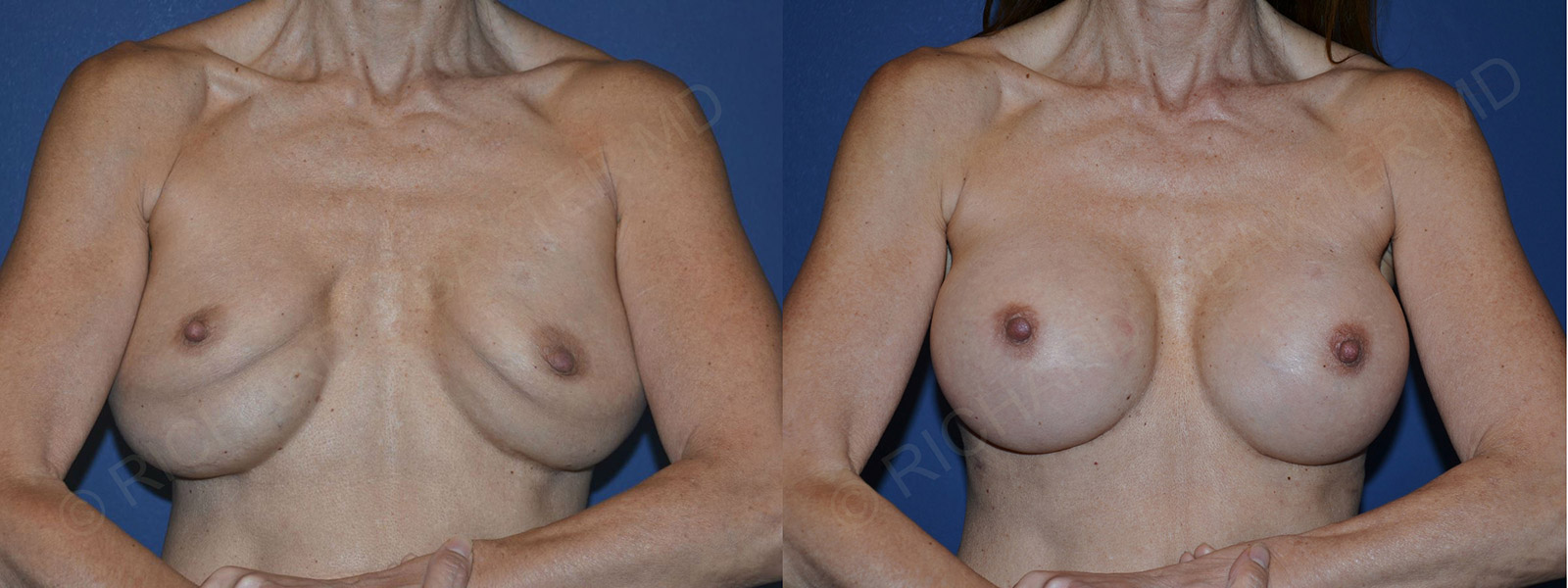
 Capsular contracture treated with capsulectomy, implant replacement, and Benellii breast lift
Capsular contracture treated with capsulectomy, implant replacement, and Benellii breast lift - If your implants are old, consider upgrading to newer versions. The gel in implants is available in more cohesive versions, and they tend to ripple less. A more natural-feeling type of saline-filled implant called the Ideal Implant is also available now, for patients who prefer saline.
- There is no one-size-fits-all solution, just as there is no one type or shape of implant that is best in every situation